Wisconsin has seen renewed debate in 2019 about legalizing medical marijuana, buoyed by bipartisan – though hardly universal – support for the move. Our analysis of medical marijuana programs across the country indicates that those programs differ in three distinct ways: who qualifies for legal purchases of medical marijuana; how its cultivation, sale, and use is regulated; and whether and how it is taxed. Those three areas also will be the key issues for state lawmakers to deliberate if they move ahead with such a proposal.
In recent years, the national conversation on legalizing marijuana has undergone a striking shift. Compared to 10 years ago, the number of states with either a medical or recreational marijuana law in place has more than doubled. Wisconsin and its surrounding states are a microcosm of the increasingly complex patchwork of state marijuana laws: while Wisconsin does not allow marijuana for recreational or medical use, two surrounding states (Illinois and Michigan) recently passed actions that fully legalize it, and a third (Minnesota) allows medical use.
Wisconsin now stands at a crossroads, with some state leaders in both parties signaling interest in a potential medical marijuana law here. With this report, the Wisconsin Policy Forum seeks to inform our state’s debate by analyzing how other states have implemented legalized medical marijuana.
Our findings suggest that—considering the paths to legalization available in Wisconsin—it is unlikely that approving medical marijuana here could quickly lead to recreational legalization, as some lawmakers have said they fear. On the other hand, we find that even if marijuana were to be legalized for medical purposes, taxed at a high rate, and left open to a wide range of potential patients, tax and fee revenue would not likely be a transformative source of revenue for the state. For those reasons, policymakers may want to consider the pros and cons of legalizing medical marijuana on their own terms rather than in the context of other major policy changes or objectives.
Under federal law, marijuana is banned as a Schedule I substance with “no currently accepted medical use.” As of early fall 2019, however, 33 states and the District of Columbia have legalized marijuana for medical or recreational use. In crafting medical marijuana laws, states have taken sharply diverging paths. After analyzing those paths, we conclude three major questions should form the basis for the medical marijuana policy debate in Wisconsin:
- Who should be eligible to participate in a medical marijuana program?
- How would those who qualify for the program be able to access the substance, and what structures should be in place to regulate this process?
- Should Wisconsin place a sales or excise tax on medical marijuana, and if so, how high should taxes be?
EXPERIENCES FROM OTHER STATES
Since the mid-1990s, 49 separate medical marijuana measures have been adopted by 33 states and Washington, D.C., including both legislation and ballot initiatives. These figures do not include the 13 states, including Wisconsin, with laws allowing very limited use of products containing CBD, or cannabidiol. These products are less controversial because they contain low levels of THC (tetrahydrocannabinol), the psychoactive substance in marijuana that gives users a “high.” As of 2018, products with a concentration of THC higher than 0.3% on a dry-weight basis remain illegal in Wisconsin, except in a few specific circumstances under a bill known as “Lydia’s Law.” The 2018 Federal Farm Bill legalized hemp (and, as a result, CBD) for commercial production, but there remain many bureaucratic hoops to jump through at both the state and federal level.

For the purposes of this analysis, we focus primarily on the experiences of the 22 states that will function as medical marijuana states at the start of 2020, although it is also helpful to consider the 11 recreational states, each of which had a medical law before legalizing adult recreational usage. As noted above, Illinois (2019) and Michigan (2018) became two of the most recent states to approve recreational marijuana. In Table 1, we summarize the major fiscal and policy components of medical marijuana laws in each of the 33 states.
Thus far, states have used one of two main routes to establish medical marijuana laws: ballot initiatives, in which a petition signed by a minimum number of registered voters allows a binding referendum to be placed on the ballot, and a majority of votes cast in the affirmative results in adoption; and laws enacted through the legislative process. In Wisconsin, only the latter option is available, as there is no ballot initiative process (constitutional amendments are passed by referendum, but only after lawmakers’ approval). This means any possible medical marijuana law would require legislative approval.
Illinois is the only state to initially approve medical marijuana through legislation that has then gone on to legalize retail sales and use by adults for recreational purposes. Vermont would be the second, but while recreational use has been approved there, state law does not yet allow for retail sales (a bill that would allow those sales is currently being considered by the state legislature). The 14 other states that initially allowed medical marijuana through legislation have not yet legalized it for recreational use.
This contrasts starkly with the experiences of states that initially passed a medical bill through ballot initiative. Of the 17 states that went through this process, nine have gone on to approve marijuana for recreational use: Alaska, California, Colorado, Maine, Massachusetts, Michigan, Nevada, Oregon, and Washington. The remaining eight adopted their medical ballot initiatives within the last decade, including five (Arkansas, Florida, North Dakota, Oklahoma, and Utah) since 2016.
This suggests the possibility that medical marijuana legalization will lead to recreational legalization may be much less of a concern in a state that does not have a ballot initiative process, as is the case in Wisconsin.
Support for recreational legalization among adults has become considerably stronger in the last two decades: according to Pew, 62% of Americans said that marijuana should be legal in 2018, doubling the percentage of those who agreed in 2000. While that may bode well for proponents of recreational legalization in states where ballot initiatives can prevail, it does not necessarily translate into support among elected officials in states where their approval is required. That is particularly the case in states, like Wisconsin, that have divided government between Democrats and Republicans or unified Republican control.
In Illinois, for example, recreational legalization was approved only after both legislative houses and the governor’s office were won by Democrats; while in Vermont, a Republican governor vetoed the first version of a bill passed by a Democratic House and Senate before signing a new bill that did not include retail sales.
There has been no indication of bipartisan support for a recreational marijuana bill in the Wisconsin statehouse, which would currently be required given the state’s divided government. Assuming, then, that medical marijuana may be the only legalization question on the table for the foreseeable future, we turn to the question of how a medical marijuana bill might define who is permitted to access the drug.
DEFINITION OF “MEDICAL” USAGE
All states that currently have legal medical marijuana programs (but not recreational) use a registry to administer the program to eligible patients. To determine eligibility, each law or ballot initiative passed in these states has defined both a “qualifying patient” and “debilitating medical condition,” generally specifying that only patients with such conditions can legally buy and use marijuana. Each of the states also requires patients to obtain a medical professional’s recommendation before gaining access to the drug, typically to confirm they have at least one of the qualifying medical conditions cited in the law or under subsequent regulatory changes. Technically, because of the federal prohibition, marijuana cannot be “prescribed,” and even with the 2018 Farm Bill, only one drug containing CBD has been FDA-approved.
A challenge for policymakers in constructing a qualifying conditions list is the scarcity of research on the possible medical benefits of marijuana. Federal law effectively constrains research that can be conducted on the drug’s potential medical uses. Still, in a meta-analysis of existing studies, the National Academies of Sciences, Engineering and Medicine (NASEM) in 2017 found “conclusive or substantial evidence” that marijuana can be effective for treating chronic pain, chemotherapy-related ailments, and chronic muscle contractions from multiple sclerosis.
The numerous medical marijuana bills passed in recent decades have cited nearly 40 distinct conditions that allow for usage of the drug. In addition to commonly cited conditions such as cancer, glaucoma, and HIV/AIDS, many bills also permit patients to use medical marijuana to alleviate symptoms like seizures or muscle spasms resulting from conditions such as epilepsy, Parkinson’s, or Tourette’s, or as an appetite stimulant for patients dealing with cancer and chemotherapy, anorexia, or Crohn’s Disease.
That said, just because several state laws include a particular diagnosis does not necessarily indicate that there are large numbers of patients who appear on state registries because of that diagnosis. In fact, our analysis finds that across states, a few conditions stand out as consistently representing a significant portion of registered patients: chronic pain and post-traumatic stress disorder (PTSD) in particular, as well as certain conditions related to cancer and chemotherapy.
For example, in an August 2019 update, the Arizona Department of Health Services indicated that nearly 90% of its qualifying patients—numbering over 180,000—listed their qualifying condition as chronic pain. Lesser but still substantial proportions were found in Rhode Island’s 2017 report (62%), New York’s 2016-2018 two-year report (73%), and Minnesota’s June 2019 update (64%).
PTSD is only listed as a qualifying medical condition in 13 states, but is associated with substantial portions of the patients on the registries in Minnesota (18%) and New Mexico (51%). Cancer—listed as a qualifying condition in nearly every state—can be listed as its own diagnosis, but patients may also be listed as having chronic pain, undergoing chemotherapy, or any number of other diagnoses depending on the physician making the recommendation and the state. Because these specific conditions define the eligibility of a large portion of registered patients, the choice of whether to include them in a medical marijuana bill or ballot can have a large impact on the number of patients participating in the program.
Another eligibility consideration for Wisconsin lawmakers relates to the ongoing opioid epidemic in the state (for more information, see 2019 Focus #15). In recent years, a number of states have chosen to explicitly or implicitly mention usage of medical marijuana as a substitute for prescription opioids in their legislation:
- Pennsylvania’s and West Virginia’s qualifying conditions include “severe chronic or intractable pain in which conventional therapeutic intervention and opiate therapy is contraindicated or ineffective.”
- Missouri’s qualifying conditions include “a chronic medical condition that is normally treated with a prescription medication that could lead to physical or psychological dependence, when a physician determines that medical use of marijuana could be effective in treating that condition and would serve as a safer alternative to the prescription medication.”
- Utah’s qualifying conditions include a physician’s determination “that the individual is at risk of becoming chemically dependent on, or overdosing on, opiate-based pain medication; or a physician determines that the individual is allergic to opiates or is otherwise medically unable to use opiates.”
Oklahoma provides an interesting case study as the only state with a medical marijuana law that does not specify qualifying conditions. Instead, its ballot initiative stated: “There are no qualifying conditions. A medical marijuana license must be recommended according to the accepted standards a reasonable and prudent physician would follow when recommending or approving any medication.” Just one year into implementation, the Oklahoma Medical Marijuana Authority announced over 178,000 participants—one of the highest totals of any state, regardless of population or how long a medical marijuana law has been in place. Compared to about 1% of the population in Vermont and 0.7% of the population in Delaware, nearly 4.5% of Oklahomans are on the state registry.
ACCESS TO MEDICAL MARIJUANA
While the eligibility definition is a major factor in determining the number of citizens who might access marijuana for medical purposes in a given state, how laws or ballot initiatives provide patient access to marijuana also plays a key role. In fact, administrative and regulatory impediments and stipulations regarding the number of allowable dispensaries by municipality or region can substantially restrict access, whether intentionally or not.
One major accessibility question concerns registry fees. Most states with a medical law in place require consumers to pay a yearly or one-time application fee to remain on the registry. The fee amount ranges from $25 in Missouri to $200 in Minnesota. Many states also allow a reduced price or waived fee to certain low-income or disadvantaged individuals. Examples include Arizona, where the $150 ID card fee is reduced to $75 for patients eligible for SNAP (i.e. federal food stamp) assistance; New Jersey, where seniors, veterans, and those on temporary or permanent disability, Supplemental Security Income, SNAP, and Medicaid see their registration fee reduced from $100 to $20; and Delaware, which halves its $50 application fee for any patient at or below 138% of the federal poverty line.
Another major accessibility question concerns the geographic availability of dispensaries. Certain states have chosen to limit the number of state dispensaries in the language of the bill or ballot initiative. For example, Delaware’s medical marijuana bill specified one “compassion center” per county in the year after the law was enacted, and an additional three centers “by 30 months after.” Vermont—whose dispensaries are only for use by medical patients—currently allows five dispensaries, with the opening of a sixth contingent on hitting a threshold for the number of patients on the state registry.
Another way that state laws can limit the number of dispensaries is to allow municipalities to prevent them from moving in, or change zoning laws to make it more difficult to open up shop. For example, Missouri’s law states that “local governments may enact ordinances or regulations not in conflict with this section, or with regulation enacted pursuant to this section, governing the time, place, and manner of operation of such facilities in the locality.” (Missouri has not yet opened its dispensaries, but has begun accepting applications.) Again, Oklahoma offers a stark contrast. That state does not limit the number of dispensaries nor allow its municipalities to reject them and has nearly 2,000 after just one year of implementation.
OTHER FORMS OF REGULATION
Should Wisconsin consider medical marijuana legislation, it would have several other regulations to consider that would impact potential usage by eligible consumers as well as public safety concerns.
For example, most states require initial application and yearly fees from marijuana-related businesses seeking to open dispensaries or otherwise participate in the medical marijuana program. New York, North Dakota, and Arizona are examples of states that charge a flat one-time application fee plus some sort of renewal fee every year or two years for any such businesses. Other states, such as Missouri, Arkansas, and Connecticut, charge different rates for producers (those that grow marijuana), processors (those that test and package marijuana), and dispensaries (retail entities that sell the product directly to the consumer). Application fees range from $250 to $55,000, and yearly renewal fees can be up to $250,000.
One significant difference between medical states is whether or not cannabis plants can be grown in the home. Especially in states with few to no dispensaries, home growing can serve as a critical legal route to acquire marijuana. Some states expressly prohibit home growing. Others allow a restricted number of plants to be grown, with 12 plants being the legal limit in a number of states. Regulations can be added on top of this. For example, certain states (Arizona, North Dakota, Nevada) only allow home growing if the dwelling is a certain distance from the nearest dispensary. Many states place a limit on the number of “mature” plants—those with usable flowers—that an individual can grow.
Another potential regulatory issue is the form in which medical marijuana can be legally purchased. In a recent statement, Republican Assembly Speaker Robin Vos signaled opposition to medical marijuana that can be smoked, stating instead that it only “should be taken in pill form.” A couple of states limit products in their dispensaries—namely, Minnesota does not sell the smokable flower of the cannabis plant. A policy limiting availability to pill form has yet to be pursued in any state.
Administratively, Wisconsin would need to consider the roles of various state agencies in a medical marijuana regulatory framework. The Departments of Justice (DOJ), Health Services (DHS), Administration (DOA), Revenue (DOR), and Agriculture, Trade, and Consumer Protection (DATCP) all have a stake in such a framework. Specific duties could be delegated to certain departments—which would require high levels of inter-agency collaboration—or all responsibilities could be delegated to one agency. Alternatively, Wisconsin could follow the lead of states like Oklahoma, Maryland, and Ohio and create a separate department devoted solely to medical marijuana administration and regulation. Currently, DATCP oversees the state’s hemp pilot program.
State law also can determine the level of protection provided to patients, growers, and suppliers. This could include protections from law enforcement—i.e., no one can be arrested by the state or a municipality for selling, growing, or using marijuana so long as they operate within the framework of the state law—as well as affirmative protections for medical users against discrimination in terms of employment, housing, custody, and other public benefits. However, federal law still applies, so no one could be protected from potential federal prosecution.
Another regulatory consideration is the extent to which a new, legal source of marijuana could serve to boost or deter a black market in Wisconsin. For example, there is a risk that individuals gaining access to medical marijuana could share their supply with family and friends, thus expanding the existing black market. Conversely, if those currently using the black market to access marijuana for medical purposes have a legal pathway to obtain the same product, then the black market could shrink. Research on the effects of medical marijuana legalization on the size of the black market is difficult to conduct, as the transactions are by their nature illegal. That said, research does show that any form of retail marijuana tends to be more expensive than black market marijuana because of licensing, regulatory compliance costs, and taxes (if applicable).
Illinois will implement recreational marijuana in January 2020. Because a considerable share of Wisconsin’s residents live within a short drive of the most populous—and therefore dispensary-dense—areas of Illinois, concerns have been raised about growth in the black market in Wisconsin and impaired driving between the two states regardless of any action Wisconsin might take to legalize the drug for medical purposes.
TAXATION AND REVENUE
The issue of how and whether to tax marijuana used for medical purposes is perhaps one of the most contentious aspects of the debate and one of the most important for all citizens given the broad-ranging fiscal implications. Unlike recreational marijuana—which for tax purposes tends to be viewed similarly to alcohol or cigarettes as worthy of an “excise” tax—the express purpose of medical marijuana is to treat a medical condition. Traditionally, most states do not apply sales taxes to pharmaceutical drugs or medications in the same way they are applied to other consumer products.
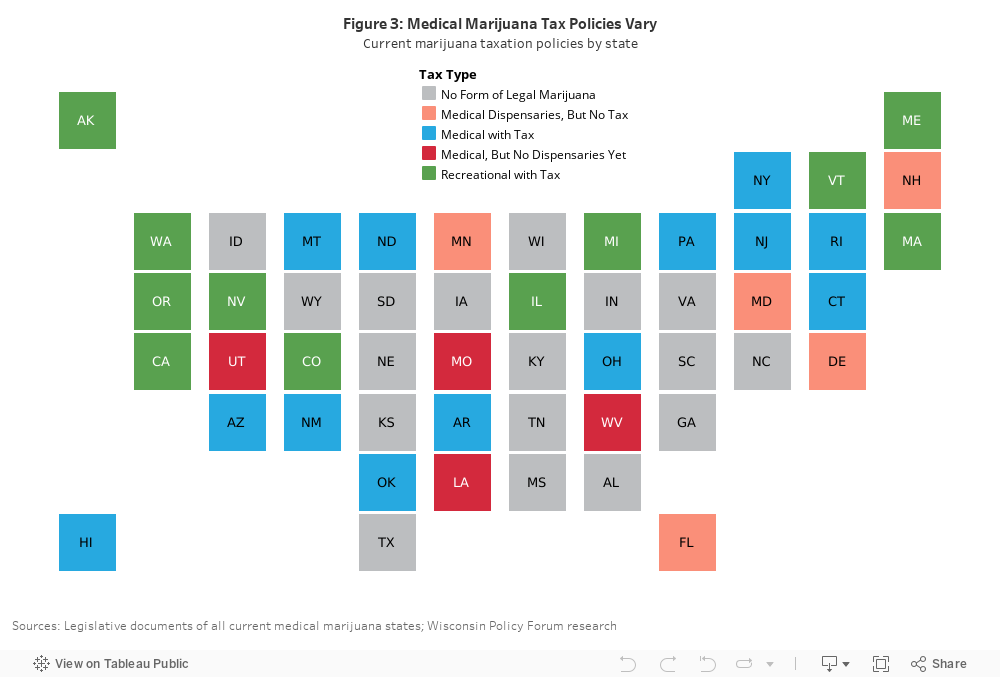
However, so far, that has not stopped many states from applying sales and excise taxes to medical marijuana. Of the 22 states with only a medical marijuana law on the books, 18 have operating dispensaries; of the 18, 13 apply some sort of sales, gross receipts, or excise tax. Two do not have a state sales tax, while the remaining three do not apply their sales tax to medical marijuana.
In most states that tax the sale of medical marijuana, regular state and local sales taxes apply. A few states, including Oklahoma, Pennsylvania, New York, and Arkansas, apply an excise tax on the producer or retailer. One issue to consider is whether a tax would be applied to multiple transactions before a final sale such as those between growers, distributors, and retailers. That could have effects such as incentivizing large, vertically integrated businesses.
While many states do not publish figures on tax revenue derived specifically from the sale of medical marijuana, insights can be gained from a few states that do:
- As mentioned previously, Oklahoma’s qualifying conditions and regulations on dispensaries are perhaps the most permissive of any medical marijuana state. In its first year of implementation, the Oklahoma Medical Marijuana Authority (OMMA) collected $15 million from patient license fees, $20.6 million from commercial business fees, and just $7.9 million from tax revenue. The state applies its 4.5% state sales tax plus local sales taxes and a 7% excise tax. The proportion of all revenue from fees may decline, however, as both business and patient application licenses decline after the first year of implementation.
- Arkansas estimated about $2.5 million annually in revenue from applying its 6.5% state sales tax to medical marijuana purchases.
- New Mexico projected a loss of about $10.8 million in revenue in FY 2020 if medical marijuana was removed from the base of the state gross receipts tax.
- Data from the Pennsylvania Department of Revenue show the state received “just over $1 million” from a 5% gross receipts tax on producers in 2018.
As can be seen with these states, the notion that revenue from the taxation of medical marijuana can be “transformational” for state budgets is misplaced, though that may not be the case for recreational marijuana. For perspective, revenue collected from cigarette taxes in Wisconsin in FY 2019 totaled $514.3 million.
Though some states that have legalized recreational marijuana devote specific percentages of tax revenue to certain prioritized budgets and programs (like youth and public health programs in Colorado), the relatively small amount of revenue generated by taxation of medical marijuana likely precludes a similar approach. Policymakers also may be reluctant to collect revenue from patients seeking treatment for a serious illness. It may be appropriate, however, to consider using medical marijuana tax revenues to offset regulatory and/or law enforcement costs associated with the program.
Another pertinent taxation issue is the extent to which driving up prices (both by implementing taxes and constricting the market in other ways) might impact the black market. Because of the piecemeal nature of the market for marijuana throughout the United States, prices tend to vary widely. Prices depend heavily on the number of producers and dispensaries in the state, how long the legal market for marijuana has existed, and—especially in medical marijuana states—what kind of market regulations the state law dictates. Prices for medical marijuana are likely to be noticeably higher than black market prices, at least initially, which could drive those who might want to purchase medical marijuana legally into the black market. The opposite scenario—many dispensaries with cheap or excess medical marijuana—could also fuel a black market, as has happened to Idaho with Oregon, a recreational state, on its border.
The medical marijuana discussion in Wisconsin should consider these issues but also must take into account the reality that any decisions will be affected by the start of sales of recreational marijuana in Illinois on January 1st of the coming year with potentially many new dispensaries.
PENDING LEGISLATION
With Speaker Vos publicly stating last summer his willingness to consider medical marijuana legislation and Democratic Gov. Tony Evers proposing medical legalization as part of his original budget plan (see the Forum’s report on the proposal here), the prospects for bipartisan action on this issue appear greater than at any time in recent memory. That said, opposition continues to be strong from certain members of the legislature, including Republican Senate Majority Leader Scott Fitzgerald.
In addition to the governor’s medical marijuana proposal, a bipartisan bill (Senate Bill 507/Assembly Bill 570) introduced by Sens. Jon Erpenbach, a Democrat, and Pat Testin, a Republican, as well as Democratic Rep. Chris Taylor, has been referred to committees in both chambers. Beyond Testin, the bill has three Assembly Republican cosponsors. Provisions of the two proposals relevant to the policy issues outlined above are summarized in Table 2.
Both the governor’s proposal and the bill introduced by bipartisan legislators include a relatively broad definition of qualifying conditions (given the inclusion of severe pain and PTSD) that would likely result in at least several thousand legal users across the state in the first few years, but neither proposal goes as far as Oklahoma’s law. Like nearly all other states with a medical law, both proposals would allow DHS to add additional qualifying conditions through rulemaking. Both proposals also include production and user fees that are in line with rates throughout the rest of the country, and both would create a registry. While Evers’ proposal included language to shield marijuana-related businesses from local zoning regulations, the lawmakers’ proposal does not.
Finally, the application of state and county sales taxes to medical marijuana sales would produce some revenue for the state: a Legislative Fiscal Bureau analysis of the Evers proposal estimated sales tax revenue of about $250,000 in year one and $500,000 in year two, plus an additional $500,000 in year one and $1 million in year two from the 10% dispensary surcharge (a provision not included in the legislators’ proposal). That said, as our analysis found, revenue from all of these taxes combined is likely to be limited, especially in the first few years of implementation. That may explain why revenue earmarks from medical marijuana taxation are unspecified in both proposals.
CONCLUSION
The high-profile medical marijuana proposals that have surfaced in the state Legislature in 2019, as well as signals of support for a medical marijuana debate from some Republican legislators, indicate its arrival in Wisconsin is no longer far-fetched. Meanwhile, legalization for medical purposes in Wisconsin appears unlikely to result in rapid recreational legalization, since Republican legislative leaders oppose it and the state lacks a ballot initiative structure similar to most other states with a recreational law in place.
Our analysis of medical marijuana laws in other states shows that if Wisconsin lawmakers do move forward with medical marijuana legislation, then their decisions on the allowable number and geographic distribution of dispensaries, as well as which conditions qualify individuals for legal marijuana usage, will have a large impact on how many citizens have access to the drug. And, for those hoping that legalization of medical marijuana will produce a windfall for state tax coffers, that hope should be tempered by the relatively low volume of sales expected from a medical program and the recognition that high taxes are arguably less justifiable for a substance used for medical purposes.
With Illinois on the cusp of statewide legalization on January 1, Wisconsin finds itself nearly surrounded by states that are expanding legal access to marijuana. Popular support for both medical and recreational marijuana legalization has been increasing rapidly since the early 2000s, and in the last 20 years, more than half of all U.S. states have moved to allow it for medical use. Whatever their individual views on medical marijuana, Wisconsin policymakers would be well-served by thoughtful review of other states’ experiences—and of their own policy goals—in considering any future changes.